
AIDS 2024 was filled with game-changing scientific breakthroughs and community-led innovations, passionate activism that called out the big issues around access to the latest advances, and the promise of renewed political commitment to sustaining an effective response to HIV – all coming together to Put people first!
The programme offered more than 40 oral abstract sessions, 50 invited-speaker sessions, 20 workshops, 17 pre-conferences, 30 symposia sessions, 100 satellite sessions and 2,200 posters. There was celebration, too: both the Global Village and the Journal of the International AIDS Society marked their 20th anniversaries.
These are some takeaways from AIDS 2024 sessions:

1. Cure:
The tone was set that this would be a groundbreaking conference for HIV cure when three people known to have been cured of HIV came together in a pre-conference. Adam Castillejo (formerly known as the London Patient), Marc Franke (formerly the Düsseldorf Patient) and Paul Edmonds (formerly the City of Hope Patient) shared their stories. Their hope was to inspire researchers and people living with HIV to keep on track to find a cure that would work for everyone.
Then came details about the “next Berlin patient”, who appears to be the seventh person cured of HIV: a 60-year-old adult male who had received a stem cell transplant for leukaemia in 2015, stopped taking antiretroviral treatment for HIV in 2018, and remains in HIV remission more than five years later. The details came with a twist: for the first time, the donor had a single, rather than double, CCR5-delta32 mutation, a genetic factor related to HIV resistance. This could have promising implications for more scalable HIV cure strategies based on gene therapy.
2. Long-acting technologies:
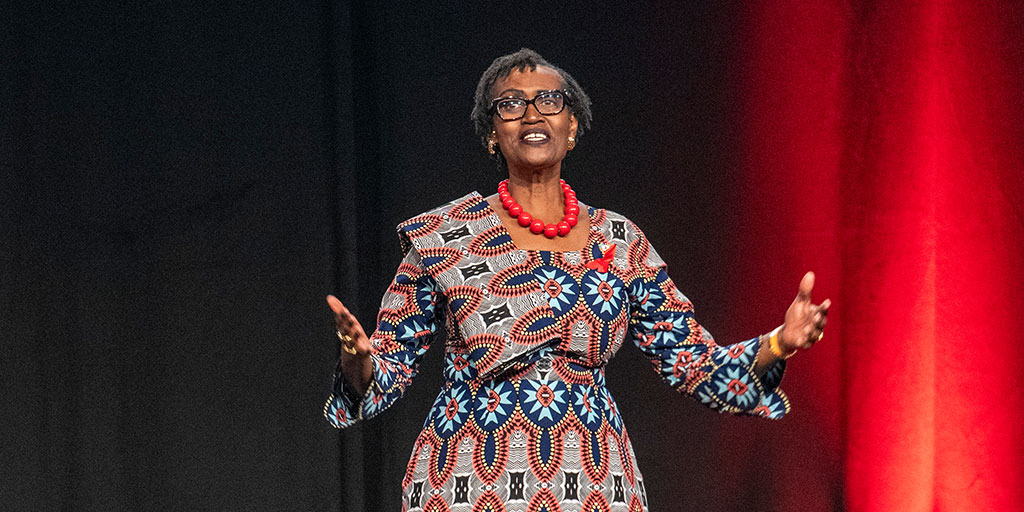
A “miracle prevention tool” is how UNAIDS Executive Director Winnie Byanyima described Gilead’s twice-yearly injectable lenacapavir for HIV prevention. Interim results from the PURPOSE 1 trial, presented at AIDS 2024, confirmed that lenacapavir gave 100% protection against HIV acquisition in cisgender women; between 1% and 2% of women using daily F/TAF or F/TDF acquired HIV.
Beyond the excitement of this game changer from science was the chanting of activists: “Shame, shame. Access for all.” Questions were raised about the pricing of lenacapavir and whether this miracle tool would be simply too expensive for use in low- and middle-income countries, such as South Africa and Uganda, where it was tested among more than 5,000 women, including pregnant women and adolescents. A study presented at AIDS 2024 estimates that lenacapavir could be priced at USD 100 per person per year and subsequently USD 35-40, with R&D investment, scaled demand and mass production of generic lenacapavir under voluntary licensing.
As outgoing IAS President Sharon Lewin pointed out in the closing session, “breakthroughs in medicine are only meaningful when the people who need those medicines can access them”.
Long-acting injectables offer a more discreet option to taking daily PrEP that also overcomes challenges in accessing daily medication. Two years ago, WHO called on countries to consider injectable long-acting cabotegravir (CAB-LA), a safe and highly effective HIV prevention option. Cost, however, is a major reason for it being kept largely out of reach in low- and middle-income countries.
So far, real-world CAB-LA implementation studies on the African continent have been lacking, and AIDS 2024 saw the release of important evidence to fill this gap. In rural Uganda and Kenya, more than half of participants in the SEARCH Dynamic Choice HIV prevention trial chose to start CAB-LA over oral PrEP or PEP. CAB-LA, the researchers say, is a popular choice for men and women, and feasible, in these settings. Long-acting HIV prevention is also a popular choice in Europe: the PROTECT survey of 8,642 men who have sex with men who are not living with HIV have a high level of interest and intention (up to 74%) to use long-acting PrEP if made available.

3. Leadership, policy and funding:
One of the biggest obstacles to realizing the vision of ending the HIV pandemic as a threat to public health and individual well-being by 2030 is a fall-off in funding. UNAIDS points to international resources for HIV in 2023 being almost 20% lower than at their peak in 2013. It says the USD 19.8 billion available for HIV programmes in low- and middle-income countries in 2023 is almost USD 9.5 billion short of the amount needed in 2025.
German Chancellor Olaf Scholz reaffirmed Germany’s strong commitment to the HIV response and announced at the opening session that Germany had become the 39th signatory to the Global Partnership for Action to Eliminate all Forms of HIV-Related Stigma and Discrimination by 2030. Closer to the conference, the Mayor of Munich called on the state of Bavaria to make drug consumption rooms legal and Munich became a Fast Track City on the conference opening day.
Over 370 Members of Parliament from over 45 countries united to put people first in rebuilding political support for ending HIV transmissions as part of the Global Parliamentary Platform on HIV and AIDS founding declaration. MPs from Argentina, Germany, the United Kingdom and Zimbabwe gathered to address the waning political commitment to the HIV response.

4. AIDS is still with us:
UNAIDS shared updated global HIV data. The data reflect the huge strides we have made, with the number of new HIV acquisitions falling by 39% globally since 2010 – and 56% in central, eastern, southern and western Africa. But there is real concern that the world will not meet the UNAIDS 2030 95-95-95 targets. The report shows that 39.9 million people were living with HIV in 2023 (from 39 million in 2022). About 1.3 million people acquired HIV in 2023 – more than three times the 2025 target of 370,000. About 630,000 people died from AIDS-related illnesses worldwide in 2023 – a death every minute and way above the 2025 target of 250,000. Against the 95-95-95 targets, progress remains at 86-89-93.
A study led by UNAIDS set out the cost of inaction and failure to meet the targets. It found that if we fail to meet the 95-95-95 targets, the human cost will include 34.9 million new HIV acquisitions and 17.7 million AIDS-related deaths from 2021 to 2050. The economic cost of inaction will be more than USD 8,200 per person in low- and middle-income countries by 2050. “The idle position is not an option,” the researchers concluded.

5. DoxyPrEP and DoxyPEP:
AIDS 2024 saw the term, “DoxyPrEP” (doxycycline pre-exposure prophylaxis to describe taking the antibiotic before sex), make its debut to join the better-known “DoxyPEP” (doxycycline post-exposure prophylaxis).
Researchers from opposite sides of the world presented findings. A trial from Canada involving men who have sex with men, living with HIV and with a history of syphilis, showed reductions of 79% in syphilis, 92% in chlamydia and 68% in gonorrhoea in the doxycycline arm compared with the placebo arm. A study from Japan among female sex workers showed a drop in STI incidence from 232.3 to 79.2 per 100 person-years. Syphilis incidence was reduced to zero; there was a marginally significant reduction in chlamydia and no significant change in gonorrhoea.
STI rates among young women using PrEP in central, eastern, southern and western Africa are high. Past research shows that DoxyPEP effectively prevents STIs among cisgender men and trans women but not cisgender women because use of DoxyPEP is low, with barriers such as side effects, pill burden, stigma and fear of partner reaction. A study on DoxyPEP adherence among young women in Kenya concluded that adherence could be better supported by decreasing frequency and urgency of dosing to allow for optimal location and timing of dosing.
A big question mark hangs over the potential for antimicrobial resistance (AMR) with the prolonged use of doxycycline. Large-scale and continued surveillance is crucial to gain further evidence around AMR.
6. Stigma, discrimination and criminalization:
These major obstacles to progress in the HIV response are not abating. On the contrary. Analysis of data from 842,169 people, including 70,109 people living with HIV, across 33 African countries links stigma with reduced engagement at every stage of HIV care. Researchers analysed three stigma measures, all associated with lower past-year HIV testing: discriminatory attitudes towards people living with HIV (reported by 36% of people); shame of associating with people living with HIV (18%); and perceived HIV stigma (79%). As community-level discriminatory attitudes increased by 50%, people living with HIV were 17% less likely to be on ART and had 15% lower viral load suppression. More than half of 18,430 healthcare workers across Europe are worried when providing care to people living with HIV. Almost half of 8,128 respondents in a study on HIV criminalization and enacted stigma in eastern Europe and central Asia had experienced stigma in healthcare settings.
Laws that criminalize LBGTQ relationships in some African countries have worsened the challenges of key populations in accessing HIV services. In Uganda, the Anti-Homosexuality Act threatens to set back progress that includes HIV prevalence among adults reducing from 18% in 1992 to 5.2% in 2020. Communities have seen a surge in discrimination, violence, arrests, “mob justice”, and service providers fearing to treat LGBTQ people. A response team (formed by government and other agencies) coordinated efforts to address the effects of the law on LGBTQ people; service providers were trained in maintaining LGBTQ-friendly services; and key population peers were supported to conduct client follow up, refills and linkages.
In Ghana, where its Parliament approved anti-gay legislation, health workers are using integrated, community-based strategies to maintain access of men who have sex with men to HIV services. This includes peer educators pivoting from group outreach to engaging one on one to reduce visibility; shifting testing and treatment to homes and safe locations; and promoting multi-month dispensing of ART and PrEP to eliminate clinic visits. As the researchers say, the influence of the legislation on HIV programming is enormous, and they call for high-level stakeholder advocacy.